


The “Healthy People” Report sanctioned by the US Department of Health and Human Services gives us a definition of Public health based on the “The Social Determinants of Health.” This definition, as I have always understood public health to be, has not been the prominent definition used on the ground and is very misunderstood if known at all. The Social Determinants of Health represent the aspects that contribute to health beyond the traditional definition of individual health that included research, disease, data, genetics, and averages. We understand now that many other factors contribute to the health of a population including access to health and mental health services, education, environment and built environment, economic stability, and social support. I add to these determinants, technology. I have tried for some time to categorize technology however I thoroughly believe it is its own area overlapping with all others.
We have been talking about these determinants for some time now, 15-20 or so years? But implementing integrated programs, services, and agencies to this point have not been super successful. In the public sector we sit in coalitions, meetings, forums, conferences and the like to try and “work together.” Perhaps I’m a victim of my instant gratification generation, but talking about the same issues for 20 years isn’t my cup of tea. We have examples of major Public Health successes, but technology has complicated systems and effective communication.
While there are examples of wrap around services, very few have mastered the level of collaboration and communication needed to move the needle on poverty and the grave health issues present today. My attention here is focused on the United States. While I have spent time researching and living abroad my expertise really lies in the interworkings of US Public Health. I don’t want to get my fellow public health professionals up in arms as we work diligently every day. That being said, it is time to have the hard and real conversations about how this work is done and who we are not serving. Public Health is intended to wrap around ALL populations in the United States. The PUBLIC. The ENTIRE PUBLIC.
I will consider expanding this article with all the data and research in my arsenal, but wanted to start with a more informal piece that is a bit easier to read (and write) based on my personal experience. Also feel free to download Healthy People 2020 info (http://www.healthypeople.gov) for a ton of national background surrounding this issue. I am also happy to share my many research papers if you contact me directly.
Access to Healthcare and Mental Health Services
For as long as I can remember, this here has been the cause of all health disparities. Faced with this argument daily in my Master of Public Health program, I decided to do extensive research to disprove this as being the best argument in this country (my fellow scientists know that research is supposed to disprove a theory, not prove it). It is still part of the issue, but not THE issue. I picked the Mexican American Female demo as my target research population based on my time working in a hospital in Mexico. This population at the time had been characterized popularly for falling victim to lack of access to care. I’m happy to share all my research with you if you’d like to contact me, but in short, it was actually the African American population at the time who actually fell near the bottom of populations who accessed care. Furthermore, my colleague found a lack of access of treatment amongst the African American population. His research was specifically in the realm of breast cancer but found that African American women had a low rate of accessing treatment.
In my research, Mexican American women accessed care (specifically women’s health care) but still had the highest fertility rate in the US. This led me to a much more in depth study of women who were accessing care but not necessarily accessing contraception. It was very difficult to find archival research that spoke to this point. My major theory was that this outcome was based on a male directed culture with fertility of a partner being an important factor to the identity of the man. I would love more research to be done in this area, but lack of culture competence in our medical system is also key. This is also by the way when I started developing my marketing theories, because what we saw in the popular media and what was true was very different.
I want to re-iterate that there are of course gaps in service. I would venture to guess that many middle class millennial peeps who do not have employer paid medical don't have insurance.Perhaps because they qualified for no assistance with an annual income that exceeds the threshold, but is still well below a living wage in California. Or perhaps because It's hardly worth paying the $240 a month for a $5000 deductible, which yes includes the basics required by law, on top of student loans, running a business, paying high tax rates, CA rents, car payments, and because and the fact that many can't actually return to their GP. Well that is certainly a situation not being talked about!? The point here is that this issue is much more complex than we want to talk about. Regardless of your opinions about health insurance, there is a clear issue here that knows no socioeconomic status, color or creed.
Education
I’m not sure I really have to explain this area, do I? I don’t have an education background but very smart people out there including Bill and Melinda Gates have a myriad of research in this area. What I can say is that our academic system in this country is incredibly broken. In my opinion it is based on memorization of facts and thinking in a way that not all of us are compatible with. It isn’t based on systems or change, it is based on “facts” and “standards” established by someone somewhere in a 30 floor office building. It has little to no bearing on cultural competency or equity. Academia is based on standardized testing, numbers, and measures that have little merit in the real world. I was blessed to have parents who prepared me for the world, but not everyone is given that opportunity. I started doing my taxes at 16, I had a credit card at 18, and managed a personal budget by 20. My mom was a business owner and my dad was a business savvy dude with amazing investment and ethics knowledge. Academia is not equal to the real world. It isn’t all bad, but broken. I am a CEO of a marketing, communications, and business development firm and have no degree in marketing, communications, or business. Thank goodness for my parents (perfect Segway to the next determinant).

Social Support
We know technology has completely changed how we define social support; however, data shows us that those populations in the US that remain close to their culture and rituals have the highest life expectancy. Specifically the Asian population has the highest life expectancy. I can’t say I agree with how “Asian” is defined, but as an average, the overarching population lives the longest. I have said for many years that the disintegration of culture in this country has caused many issues for its residents. How many American kids wake up saying, “who am I and where did I come from?” My generation travels more than any other which I feel is incredibly promising, but so many still live in isolation and without the necessary support to be successful. We as humans want to be a part of SOMETHING which sometimes leads us to unhealthy associations and situations. Social support looks different to all of us and can come in the form of family, clergy, friends, clubs, etc. These social support entities help us learn to communicate, collaborate, feel wanted, feel needed, and feel we have a place in life. Knowing we have a place in this crazy world can make all the difference.
Environment and Built Environment
This is by far one of the most overlooked areas in public health. It isn’t greatly understood by public health professionals outside of the green building, sustainability, and environmentalist realm. We do have a lot of environmental scientists and engineers at the table especially when it comes to water, transportation, and the like but the fields still seem to be miles apart in the day to day. I have had the privilege of once in my life experiencing someone saying they “worked in public health” as an adviser to the US Department of Energy, but I assure you I was in momentary shock when I heard this. While research dates back 20+ years regarding the health implications of living in old, asbestos filled public housing on the East Coast, we somehow forget how important our environment is to our health.
In short, the conversation needs to become more prominent between housing experts, renewable energies (and dirty energy), environmental scientists, and public health professionals. Here in the Northbay we have a huge amount of alternative energy companies, none of which are ever in the meetings I’m sitting in about health equity or public health. I know some cities and counties are ahead of us here in the Northbay including San Francisco City and County, but we all need to take notes. You will hear me preach on the regular for more private/public partnerships. The private sector HAS to be at the table. Giving money is not enough. Charity is not enough.
Economic Stability
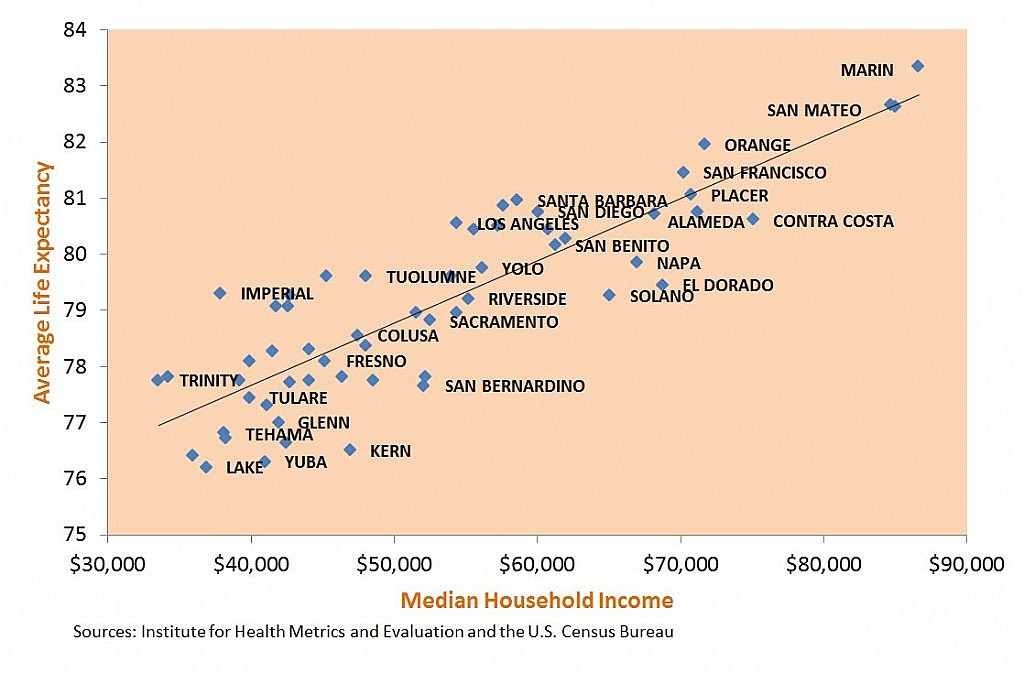
This is another area that I feel needs little to no explanation. If you have not heard that “place matters” it is time to step out. We know that where someone lives greatly affects how long they will live. Along with the environmental implications of where someone lives, their income also plays a huge part. This fact goes alongside environment and built environment and is very relevant. Economic stability in this country is key to any sort of health stability. Money may not buy happiness but it does by healthcare services, education, technology, a better environment, and associations. Economic stability is relative to the individual but we know that those who are employed have better outcomes across the board.
Technology
Stephen Hawking believes technology creates inequity, so in my mind it has to be its own social determinant of health (he is pretty smart if you didn’t know). I think it is clear to everyone at this point that access to technology varies based on physical location, economic status, education level, and even culture or ethnicity (I’m not a huge fan of how we breakdown ethnicity in this country so I am always looking for another way to describe populations, so maybe culture?). Lack of access to technology whether it be advanced medical technologies to a smart phones to STEM classes, a person’s wellbeing is affected by access to technology this country. Our communication system is now built on technology for better or for worse. Bridging the gap to access and refraining from underestimating our “low opportunity” populations are a couple of the keys to success in this area of public health.
The major barrier is that the “public health” sector as we traditionally know it, run by government, is WAAAAYYYY behind on technology issues. We have all seen the major tech failures of our local, state, and national government levels (without naming any names). At the same time we, public health professionals, are supposed to compete with the major enterprises, some of which hurt the public health of our country and have multimillion dollar technology and marketing budgets. Somehow for better or worse private companies get it and public entities do not. This is the first gap that needs to be addressed. We cannot keep working in these little silos fighting for funding to use poorly constructed or implemented technologies. Does that statement make you uncomfortable? It should. I won’t even get into a rant about government contracting processes here, but something needs to be done. Mark Zuckerberg created the beginnings of Facebook in a dorm room and Steve Jobs conjured up a premise for a major OS in a garage, but somehow it takes 10 tries to get logged into the IRS portal which I can guarantee you cost tens of thousands if not hundreds of thousands of dollars.
A note for the dreamers
What I know is that systems have to be in place to help these sectors collaborate and make change. It is a difficult situation, but a necessary one to address. All the brilliant experts who sit in these various areas need to come together. And it is beyond possible that we can make change. The good news is that as the Founder & CEO of MaberMe, Inc. I am actively looking to start building bridges and addressing gaps. We are all in this together.
